
Opioid-Induced Constipation (OIC) Bowel Function Index Calculator
Assess Your Constipation Severity
The Bowel Function Index (BFI) is a simple 3-question tool to assess the severity of your opioid-induced constipation. A score above 30 indicates you likely need treatment. Use this tool to track your symptoms and discuss with your doctor.
Your Bowel Function Index Score
The Bowel Function Index helps you and your doctor understand the severity of your constipation. A score above 30 suggests you may need treatment.
If your score is above 30, talk to your doctor about: - Starting an osmotic laxative like PEG - Adding stimulant laxatives if needed - Considering prescription PAMORAs if standard treatments aren't effective
When someone starts taking opioids for chronic pain, they often focus on how well the medication controls their discomfort. But there’s a side effect that rarely gets talked about until it becomes unbearable: opioid-induced constipation (OIC). It’s not just a mild inconvenience. For 40% to 60% of people on long-term opioids, it’s a persistent, frustrating, and sometimes dangerous problem that doesn’t go away with time - unlike nausea or drowsiness, which often fade. If you’re on opioids and struggling to have a bowel movement, you’re not alone. And more importantly, you don’t have to suffer through it.
Why Opioids Cause Constipation
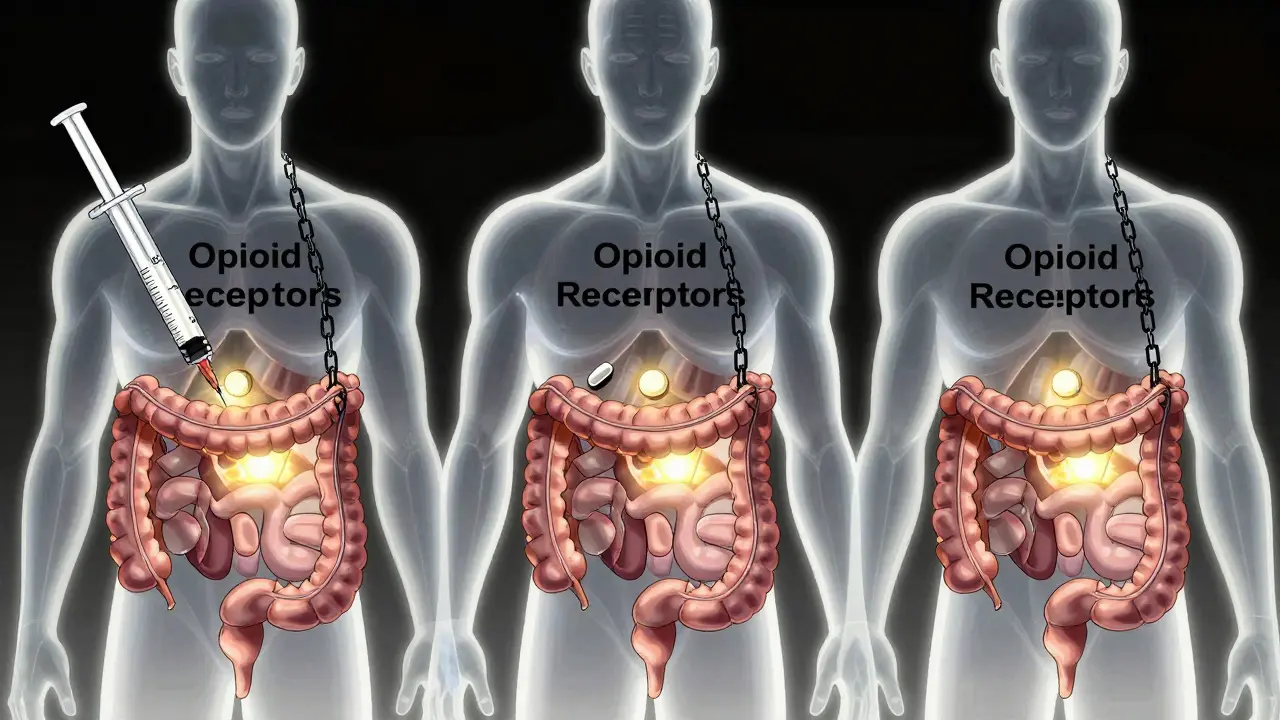
Opioids don’t just affect your brain. They bind tightly to μ-opioid receptors in your gut, slowing down everything from stomach emptying to colon movement. This leads to three big problems: your intestines move slower, your stool gets harder as more water is absorbed, and your anal sphincter tightens up, making it harder to push out even soft stool. The result? Straining, bloating, a feeling of incomplete emptying, and sometimes severe pain or blockage.
Unlike regular constipation, OIC doesn’t improve with diet or time. It’s built into how opioids work. That’s why typical advice like “eat more fiber” or “drink more water” often falls short. You need targeted solutions.
Prevention Starts on Day One
The biggest mistake doctors and patients make? Waiting for constipation to happen before doing something. Studies show that starting a laxative on the same day you begin opioids prevents 60% to 70% of severe cases. Don’t wait until you’re in pain or haven’t had a bowel movement in four days. Be proactive.
Here’s what works best from day one:
- Polyethylene glycol (PEG) - an osmotic laxative that pulls water into the colon without irritating it. It’s gentle, safe for long-term use, and works better than stimulant laxatives for OIC.
- Stimulant laxatives like senna or bisacodyl can be added if PEG alone isn’t enough. They help trigger contractions in the colon, but shouldn’t be used alone.
- Hydration and movement - drink at least 2 liters of water daily and walk 20 minutes twice a day. Even light activity helps stimulate bowel function.
Pharmacists play a huge role here. When a patient gets an opioid prescription, a simple conversation about bowel health can increase proper laxative use by 43%. If your pharmacist doesn’t bring it up, ask. You’re not being difficult - you’re being smart.
When Laxatives Aren’t Enough
Over 68% of patients on opioids say standard laxatives don’t fully help. If you’re still struggling after a few weeks of consistent use, it’s time to consider prescription options: peripherally acting μ-opioid receptor antagonists (PAMORAs).
PAMORAs are designed to block opioids from acting in the gut - without touching the pain relief in your brain. They’re not magic pills, but they’re the most effective option when laxatives fail.
Here are the three main ones:
| Medication | Form | How Often Taken | Key Benefits | Common Side Effects |
|---|---|---|---|---|
| Methylnaltrexone (Relistor®) | Subcutaneous injection | Daily or every other day | Works in under 30 minutes; approved for advanced illness and palliative care | Abdominal pain (28%), dizziness |
| Naldemedine (Symproic®) | Oral tablet | Daily | Reduces constipation and may prevent opioid-induced nausea; FDA-approved for chronic non-cancer pain | Abdominal pain (19%), diarrhea |
| Naloxegol (Movantik®) | Oral tablet | Daily | Effective for long-term use; improves stool consistency | Abdominal pain (22%), headache |
These medications are game-changers for many. One patient on Reddit said, “Relistor injections work within 30 minutes when nothing else does.” Another wrote, “Naldemedine has allowed me to stay on my pain medication without constant bathroom struggles.”
But they’re not perfect. About 28% of users report abdominal pain. And cost is a major barrier - they range from $500 to $900 a month without insurance. Many insurance plans require prior authorization or force patients to try cheaper laxatives first, even when those have already failed.

Who Should Avoid PAMORAs?
Not everyone can use PAMORAs. They’re contraindicated if you have a known or suspected bowel obstruction. That includes people with recent abdominal surgery, severe inflammatory bowel disease, or a history of intestinal blockages. There’s also a small but real risk of gastrointestinal perforation - a tear in the gut lining - especially if the bowel is already inflamed or damaged.
Dr. Jane Smith, a gastroenterologist at Mayo Clinic, puts it plainly: “PAMORAs are powerful, but they’re not safe for everyone. We need to screen carefully.”
If you’ve had abdominal surgery in the last 6 months, or if you have Crohn’s disease or diverticulitis, talk to your doctor before starting a PAMORA. The risks aren’t zero, and they need to be weighed against your quality of life.
What About Lubiprostone?
Lubiprostone (Amitiza®) is another option. It works differently - it activates chloride channels in the gut lining, pulling fluid into the intestines and softening stool. It’s FDA-approved for women with chronic idiopathic constipation and OIC, but studies show it works just as well in men. The catch? About 1 in 3 people get nausea. It’s not a first-line choice, but for some, it’s a useful alternative.
Real-World Challenges
Despite the science, OIC is still undertreated. Only 32% of primary care doctors routinely prescribe bowel management with opioids. In palliative care, it’s 85%. That gap is huge. Why? Many doctors don’t know the guidelines. Patients are afraid of taking “another pill.” And insurers make access hard.
Here’s what you can do:
- Ask your doctor: “Should I start a laxative with this opioid?”
- If you’re on opioids for more than two weeks and haven’t had a bowel movement every 2-3 days, speak up.
- Keep track of your bowel habits using a simple log: frequency, effort, stool consistency (use the Bristol Stool Scale).
- Ask for the Bowel Function Index (BFI) - a simple 3-question tool. A score above 30 means you need treatment.
And if your insurance denies coverage for a PAMORA? Appeal. The American Society of Gastroenterology says inadequate OIC management costs the U.S. system $2.3 billion a year in ER visits, hospitalizations, and lost productivity. That’s not just a medical issue - it’s a systemic failure.
What’s Next?
The field is moving fast. In 2023, a once-weekly injection of methylnaltrexone got FDA approval. That’s a big win for people tired of daily shots. And by 2026, researchers expect to see personalized OIC treatment based on genetic markers - meaning your doctor could test your DNA to predict which laxative or PAMORA will work best for you.
For now, the message is clear: OIC is common, serious, and treatable. You don’t have to live with it. Start with PEG and movement on day one. If that fails, ask about PAMORAs. Don’t accept “it’s just a side effect” as an answer. Your quality of life matters as much as your pain control.
Is opioid-induced constipation the same as regular constipation?
No. Regular constipation often improves with fiber, fluids, and exercise. OIC is caused by opioids directly slowing gut movement and tightening the anal sphincter. It doesn’t respond as well to lifestyle changes and usually needs targeted medication like osmotic laxatives or PAMORAs.
Can I just use over-the-counter laxatives forever?
You can, but they often don’t work well enough for OIC. Many patients need to combine osmotic laxatives (like PEG) with stimulant laxatives. If you’re still struggling after 2-4 weeks of consistent use, it’s time to talk to your doctor about PAMORAs. Waiting too long can lead to fecal impaction or bowel obstruction.
Are PAMORAs safe for long-term use?
Yes, for most people. Methylnaltrexone, naloxegol, and naldemedine have been studied for years in patients on chronic opioids. The main risks are abdominal pain and diarrhea. The biggest concern is for people with bowel obstructions or recent surgery - those groups should avoid them. Always discuss your medical history before starting.
Why are PAMORAs so expensive?
They’re brand-name drugs with limited competition. Without insurance, they cost $500-$900/month. Many insurers require step therapy - meaning you must try cheaper laxatives first, even if they’ve already failed. Some patient assistance programs exist through manufacturers. Ask your pharmacist or doctor about them.
Can I take PAMORAs if I have cancer?
Yes - and in fact, the American Society of Clinical Oncology (ASCO) recommends naldemedine for cancer patients starting regular opioid therapy. It not only treats constipation but may also reduce opioid-induced nausea and vomiting. It’s one of the few treatments with specific cancer guidelines behind it.
What should I do if I haven’t had a bowel movement in 5 days?
Don’t wait. Contact your doctor immediately. Going more than 5 days without a bowel movement on opioids increases your risk of fecal impaction or bowel obstruction. You may need an enema, manual disimpaction, or urgent PAMORA treatment. Never use harsh laxatives or enemas without medical advice if you’re on opioids.
Final Thought
Opioid-induced constipation isn’t something you have to live with. It’s a predictable, preventable, and treatable side effect. The tools exist. The guidelines are clear. What’s missing is action - from doctors, patients, and insurers. If you’re on opioids, make bowel health part of your care plan from day one. Ask questions. Push for help. Your body deserves more than silence.
Been on opioids for sciatica for 3 years. PEG was the only thing that kept me from becoming a human brick. Started it day one like they said - no regrets. My GI doc was surprised I didn’t wait till I was in agony. Seriously, just do it. Your colon will thank you.
It is a matter of profound philosophical inquiry that pharmaceutical interventions, while efficacious in mitigating the physiological sequelae of opioid administration, simultaneously perpetuate a systemic reliance on pharmacological correction rather than addressing the ontological dilemma of chronic pain management itself. One must ask: are we treating the symptom, or merely postponing the inevitable confrontation with the body’s intrinsic limitations?
I’m a nurse and I can’t tell you how many patients I’ve seen who didn’t know OIC was a thing until they were hospitalized for impaction. Seriously, if you’re on opioids, ask for a bowel plan. It’s not weird. It’s basic care. Pharmacists? They’re your secret weapon. Talk to them.
So let me get this straight. You’re telling me the solution to being constipated from painkillers is… more pills? And we’re supposed to be impressed? Cool. Next you’ll tell me the cure for hangovers is more alcohol.
That PAMORA table is gold. Naldemedine’s the one I’d pick - daily pill, helps with nausea too. But man, the cost is insane. I had to appeal twice just to get my script covered. Insurance wants you to suffer first. Classic.
They don't want you to know this but the government is using opioids to control the population. Constipation is just the first step. Next they'll make you poop in a tube. I saw a video. Look up Project Lax. It's real.
Why are people so lazy? Just eat more fiber drink water move around. Stop asking for magic pills. You want to be healthy? Do the work. This whole thing is just another example of modern medicine coddling people.
I started PEG on day one after my back surgery. My husband said I was overreacting. Then I didn’t have to use a suppository for 6 weeks. It’s not complicated. Do the thing. Your body will thank you later.
Ugh. Another article that treats patients like children. You don’t need a table. You don’t need a 3000-word guide. You need to stop being so passive. If you’re constipated, go to the bathroom. Try harder. It’s not rocket science.
From India we have similar issues but access to PEG is limited. Most use senna but it causes cramps. We need low-cost alternatives. The science is solid but delivery is broken. Hope this changes soon.
You got this. OIC is annoying but it’s solvable. Start with PEG. Walk. Hydrate. Talk to your pharmacist. You’re not alone. Millions are doing this right now - you’re one step away from relief.
My mom’s on morphine for metastatic cancer. Naldemedine changed her life. She could finally eat without nausea and go to the bathroom without crying. I wish everyone knew this existed. It’s not just about comfort - it’s about dignity.